[ad_1]
In the suburbs of Maryland, Dr. Jeffery Dormu’s presence is hard to miss. He’s a regular on the local TV station, which has featured him and his practice five times over the past five years. And he smiles down from an electronic billboard outside a three-story vascular center he calls The Watcher. “It has a biblical reference, which is to watch over the community,” he said at its 2018 opening. In response to the country’s “tragedy of cardiovascular disease,” the center trademarked the phrase “vascular devastation,” a slogan frequently invoked in its marketing, along with a claim to have “saved over 34,000 lives and limbs.”
Dormu and his group, the Minimally Invasive Vascular Center, have been a magnet for people with leg pain who worry they have peripheral artery disease, a condition that afflicts more than 6.5 million Americans and happens when fatty deposits narrow the arteries and block blood from flowing to the legs.
But Dormu’s portrayal of his practice as a heroic refuge hid a distressing statistic: The vascular surgeon was performing an invasive leg treatment more often than almost any other doctor in the country, even when his patients didn’t need it and even as evidence of harm mounted.
One man had to have his leg amputated after Dormu administered multiple invasive treatments for mild pain, according to legal filings. A 62-year-old grandmother bled out and died shortly after Dormu cut into her, according to another lawsuit.
Dormu’s go-to procedure, the atherectomy, involved shaving blockages with blade-topped catheters. Best practices recommend that doctors hold off on invasive procedures like these, which can lead to complications including limb loss, on patients in the earliest stages of disease; doctors should first see how the patients do with exercise and medication. Dormu defaulted to atherectomies almost immediately, patient legal and medical records show.

Credit:
Shuran Huang for ProPublica
Four years ago, leading researchers warned the Centers for Medicare and Medicaid Services that some doctors were potentially abusing interventions. The researchers implored the government insurer to scrutinize its own data to identify overuse, noting that some of the doctors could present an “immediate threat to public safety.”
There is no public evidence that CMS meaningfully responded.
But a ProPublica analysis of CMS data suggests that if the agency had reviewed its own figures, it would have discovered that Dormu was part of a small pool of physicians performing a disproportionate number of treatments. From 2017 to 2021, the analysis shows, the top 5% of doctors conducting atherectomies — about 90 physicians overall — accounted for more than a third of all procedures and government payments, totaling nearly a billion dollars.
Near the top of the list sits Dormu, logging more atherectomies — and making more money from them — than almost every other doctor in America.
CMS paid Dormu more than $30 million in the past decade for vascular procedures he performed on hundreds of patients.
Dormu declined to be interviewed and did not respond to emailed questions.
But a chorus of experts told ProPublica that the federal government’s decision to provide unconditional payments for vascular procedures — and then not pay attention to what happened — is a prime example of what’s wrong with the American health care system.
“The government is really to blame for setting these tremendously high reimbursement values without looking into whether these procedures are helping people or are just worthless procedures or, in fact, are hurting people,” said Dr. Dipankar Mukherjee, a vascular surgeon and chief of vascular surgery at Inova Fairfax Hospital in Virginia.
CMS kicked off the problem 15 years ago, when it tried to rein in the swelling hospital costs for vascular care. Over the past few decades, advances in technology allowed patients with serious circulation problems to avoid open surgery and instead undergo minimally invasive treatment with cutting-edge devices. As they flocked to hospitals for these procedures, patients with clogged leg arteries became even more expensive than patients with clogged heart arteries.
In 2008, recognizing that the procedures could be done safely and more efficiently outside hospitals, CMS officials turbocharged payments to doctors’ offices that deployed balloons and stents to widen arteries. And in 2011, they began to reimburse those offices for atherectomies.
Before the change, an office provider inserting a stent could make about $1,700 from Medicare; deploying a balloon could bring in roughly $3,800. By 2011, the payments rose to about $6,400 and $4,800 respectively. But nothing compared to the payout for atherectomies conducted in offices: about $13,500 per procedure, as opposed to roughly $11,450 in a hospital.
Instead of saving money, the government started a boom.
Atherectomies increased by 60% from 2011 to 2014; Medicare’s overall costs for peripheral vascular treatments climbed by nearly half a billion dollars, or 18%.
The government insurer didn’t change course in 2014, when research began to indicate that atherectomies may not be more effective than cheaper alternatives, or in 2019, when experts warned the procedure may be associated with a higher risk of complications.
From 2013 to 2021, the most recent year of Medicare data, the number of atherectomies has doubled and payments to doctors have nearly tripled, totaling about $503 million in 2021.
“There’s definitely places where atherectomy is very helpful,” said Dr. Caitlin Hicks, an associate professor of surgery at Johns Hopkins University School of Medicine. “But it’s definitely being used inappropriately, and that’s when bad things happen.”
Experts fear patients are being caught up in a new era of profit-driven procedure mills, in which doctors can deploy any number of devices in the time it takes to drill a tooth and then bill for the price of a new car.
The generous reimbursements have created a conflict of interest for doctors running their own practices, who are supposed to make unbiased medical decisions while also being responsible for a lease, overhead and staff. And unlike hospitals, which have panels and administrators who spot adverse events and questionable billing, these offices don’t face such scrutiny.
CMS, experts say, should step up: It could reduce its reimbursements or even investigate doctors with outsized procedure patterns.
ProPublica reached out to CMS more than two weeks ago, listing the facts in this story, asking questions and requesting an interview. CMS did not make an official available to talk or provide any written answers.
“Vascular medicine now is the frontier of the Wild West,” said Dr. Marty Makary, a professor of surgery and health care quality researcher at Johns Hopkins University School of Medicine. “People are flying blind walking into the clinics of these doctors with egregious practice patterns, and we know that their pattern is indefensible.”
It was at the cusp of this lucrative new era in vascular medicine that Dormu, an ambitious young doctor from Washington, D.C., entered the scene.
After earning his medical degree at the New York Institute of Technology College of Osteopathic Medicine and completing an additional eight years of training in New York and New Jersey hospitals, including a residency in general surgery and two fellowships in cardiothoracic and vascular surgery, he received his license to practice medicine in Maryland in 2007. That year, he founded the Minimally Invasive Vascular Center.
“People in general are just afraid of surgery,” he later told a local TV journalist. “They can get by with minimally invasive surgery, a needle puncture without having to be cut, without having to worry about an amputation. They walk in and within hours they walk out, and pretty much healed.”


Credit:
Shuran Huang for ProPublica
Dormu opened several vascular offices in the region. At one point, his group also partnered with the Washington, D.C., Department of Aging and Community Living, providing hundreds of free vascular screenings for elderly patients at senior centers and residences across the capital.
But according to public records and lawsuits, as his profile and his practice grew, so, too, did evidence of harm.
In March 2016, while he was performing an elective aorta repair at Providence Hospital, the patient began to hemorrhage, according to a District of Columbia Board of Medicine document on the incident. After trying to control the bleeding, Dormu transferred the patient to the intensive care unit for resuscitative efforts and then left the hospital for his private practice and other appointments.
He was gone for more than two hours, and in that time, hospital staff couldn’t reach him. The hospital patient died in the recovery room from hemorrhage and organ failure, the report said. Six years later, the District of Columbia Board of Medicine would reprimand him for the incident alongside a $5,000 fine, finding that he abandoned a patient in need of further emergency care, “knowing the high risk of mortality and without adequate communication to other hospital staff.”
The death of the patient did not interfere with his medical license or appear to slow his career.
Nine months later, a mechanic sought his care for mild leg pain. As the owner of his shop, Steve Rosenberg clocked long hours, six days a week, repairing anything with wheels or an engine. But as he reached his mid-50s, the long days of standing under vehicle lifts had begun to strain his legs.
His primary care doctor suggested that he see a vascular specialist and handed him a list of physicians to choose from. Dormu happened to have an office in the same plaza as Rosenberg’s auto shop, between a jujitsu studio and a dentist’s office.
He first visited Dormu’s practice that December.
Instead of starting with more conservative treatment, Dormu deployed a trifecta of interventions on both of Rosenberg’s legs within three months, widening his arteries with stents and balloons, and debulking his vessels with atherectomy devices, according to later legal filings.
Shortly after one of the procedures, Rosenberg’s left foot grew numb and was cool to the touch. He went to the emergency room, where doctors discovered that one of his stents had clogged, hindering his vessel from carrying blood.
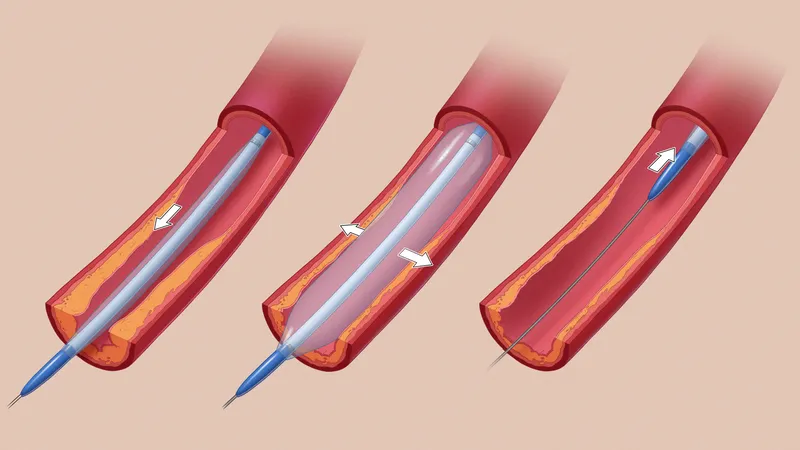
Angioplasty: A compact balloon is inserted into a blood vessel and inflated to flatten plaque against its walls.
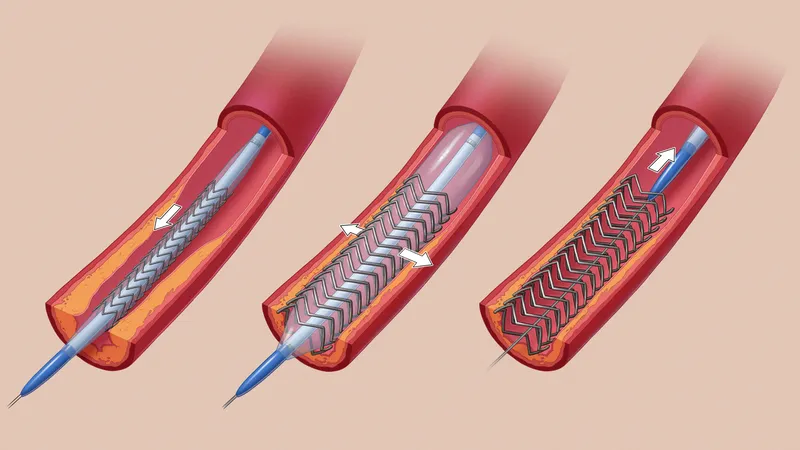
Stent: A metal mesh tube is implanted into a narrowed blood vessel to hold open its walls.
Atherectomy: A catheter, often capped with a blade or laser, is inserted into a blood vessel and removes plaque off its walls.
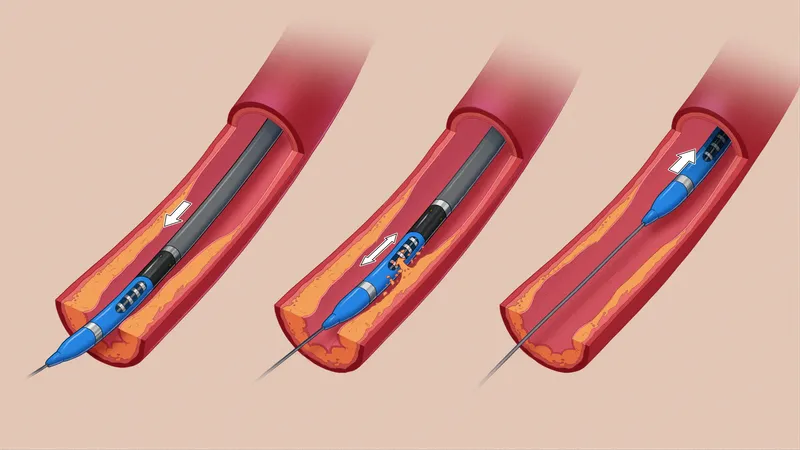
Credit:
Illustrations by Now Medical Studios, special to ProPublica
Dormu called him back to his office, where he repeated the procedures: shaving the blockages, ballooning the artery walls and installing another stent.
The next day, he repeated the procedures again, ballooning his vessels and installing yet another stent.
Dormu sent Rosenberg to Providence Hospital in Washington, D.C., for further treatment. Within a day, his left foot had grown cold, a sign that blood likely no longer flowed freely through his vessels.
According to the terms of a legal settlement in a malpractice suit against Dormu, Rosenberg cannot comment on his care. However, public documents filed in his case, including assessments from medical experts, illuminate the cascade of procedures and the outcome.
A vascular surgeon Dormu retained for his defense, Dr. Garry Ruben, said the interventions were warranted; he said Rosenberg had been prescribed an anti-platelet medication, which he did not consistently take. In legal filings, Dormu blamed Rosenberg’s injuries on his preexisting medical conditions and circumstances outside his control.
However, after reviewing medical records and diagnostic studies, Dr. Christopher Abularrage, an expert retained by Rosenberg and a professor at Johns Hopkins who specializes in vascular and endovascular surgery, found several “breaches of the standard of care.” Dormu had failed to prescribe conservative therapy and lifestyle modifications first, he found, and “persisted with unindicated, endovascular interventions in the face of persistently poor outcomes and diminishing returns.”
In less than six months, Rosenberg had been transformed from a patient with mild leg pain to one with a high risk of limb loss, he concluded.
Rosenberg spent nearly a week at Providence Hospital, the life slowly draining from his leg, before he was transferred to Washington Hospital Center on April 8, 2017, according to records. By then, his left leg was gangrenous and had no pulse. All of the stents had become blocked.
Without better options, doctors amputated his leg.
Between 2013 and 2017, Dormu earned about $14.5 million from Medicare — more than 99% of other vascular surgeons across the country — for treating hundreds of patients a year, the vast majority of them in his clinics.
In 2018, he was able to afford an upgrade.
The Watcher was not like other surgical centers. In its entrance stood a juice bar that could serve organic cold-pressed drinks to patients. Crystal chandeliers adorned its hallways. Moist air was pumped through its vents. And more than a dozen original modern paintings lined its walls, making it feel like an art gallery. “We wanted it to give that shock and awe,” Dormu said in a video interview from the facility’s opening day.

Credit:
Shuran Huang for ProPublica
His clinic provided a litany of medical services, including treatments for uterine fibroids, erectile dysfunction and varicose veins, as well as elective nonsurgical fat reduction.
The expansive facility boosted Dormu’s earnings. From 2018 through 2021, he earned nearly $18 million in Medicare payments for all of his clinic’s activities.
One procedure stood out from the rest: Nearly $12 million of that came from atherectomies, according to Medicare data.
He performed one on Alice Belton, a high school nursing teacher who sought help in 2018 for lower extremity pain, numbness and tingling. Her artery blood flow was normal; even Dormu noted that she didn’t have severe leg pain, according to an ongoing lawsuit. And yet, he conducted multiple procedures over about a year, shaving plaque, ballooning her vessels, treating her veins and running invasive scans; the procedures were unnecessary, according to a medical expert retained in her case.
Belton says she has since developed permanent nerve damage in her leg, which has prevented her from working full time. In legal filings, Dormu denied the allegations and claimed that the alleged injuries were caused by preexisting conditions.
“The experience with Dr. Dormu has shaken my confidence in health care practitioners and more importantly in myself,” she said. “I feel duped that this surgeon convinced me, a nurse, that my problems required such radical surgical interventions.”
And then there was John Malinich, who had no leg pain but wanted to get his circulation checked in 2019 after he saw Dormu’s billboard. At first, Malinich didn’t question Dormu’s treatments; the doctor’s confident demeanor and lavish facility impressed him and put him at ease.
“After surgery on both of my legs, they wanted me to go back and do it over again,” he said. “After that, I started getting suspicious.”
He said he got a second opinion from another vascular surgeon who informed him that the prior procedures, which involved balloons, an atherectomy and a stent, had been unnecessary. To ensure his stent doesn’t collapse or clog, doctors now have to annually monitor Malinich. He filed a lawsuit against Dormu, who has denied allegations of overtreatment. The case is ongoing.
“I trusted the guy,” Malinich said. “But it was just to make money.”
The next year, Heather Terry was looking forward to her mother’s return home after a six-month stint rehabilitating in a nursing home. For years, Heather had helped take care of 62-year-old Linda Terry, who had debilitating epilepsy. After a fall down a flight of stairs and subsequent back surgery, Terry was left paraplegic and unable to walk.
Just before she was supposed to be discharged from the nursing home in August 2020, the staff told Heather Terry that her mother had leg pain and ulcers on her heels that needed treatment. According to her family, Linda Terry had no prior circulation issues. The procedure was simple, the staff said, and would be conducted in a clinic just down the road.
On Aug. 13, Terry was transferred to Dormu’s center, where he started an atherectomy procedure, inserting the small tube capped with blades into her vessels to shave the plaque from her artery walls.
Less than 15 minutes into the treatment, her blood pressure began to drop.
With atherectomy, there’s always a risk that the device may dissect the vessel, which would require immediate care.
Dormu aborted the procedure and brought Terry into the recovery area. She was drowsy and her blood pressure continued to waver, signs that she may have been bleeding internally, according to her family’s attorney. Instead of being rushed to the emergency room, legal filings show, she was sent back to the nursing home, where she became unresponsive.
The nursing home called an ambulance, which ferried her to the emergency room at the University of Maryland Laurel Medical Center. Three hours later, she was pronounced dead, according to the lawsuit, a consequence of severe anemia due to internal blood loss.

Credit:
Michelle Gustafson, special to ProPublica
For the aborted procedure, according to the family’s attorney, Dr. Zev Gershon, Dormu charged her insurance about $20,000.
Heather Terry believes that if Dormu had treated her mother with appropriate care and transferred her directly to the hospital, she might have survived. “It went from ‘She’s going to come home tomorrow’ to ‘She’s dead,’” said Terry, whose ongoing malpractice case against Dormu is set to go to trial this year.
In legal filings, Dormu denied any involvement in her mother’s death. He said in a deposition that he did not see evidence of bleeding and that Linda Terry’s anemia could have been due to a prior fall. He said he also gave a directive to send her to the hospital after the aborted procedure, despite EMS records obtained by the family’s attorney showing that Terry was sent back to the nursing home.
“I trusted doctors,” Heather Terry said, “but now I’m starting to think that maybe they shouldn’t be as fully trusted.”

Credit:
Michelle Gustafson, special to ProPublica
By 2021, Dr. Kim Hodgson, a former president of the Society for Vascular Surgery, recognized that unfettered profiteering in his field was not just a threat to patients, it also stood to damage the credibility of his speciality. Notably, abuse in outpatient vascular facilities was the No. 1 complaint he had received from members. That August, the vascular surgeon stood before hundreds of doctors at the society’s annual conference and made a plea.
“Somebody has to address what should never have been allowed to get to this level of threat to us and our patients in the first place,” he said. “We can play whack-a-mole every time the bad actors surface until the cows come home, but that leaves a trail of harmed patients and wasted resources.”
In dozens of slides, he laid out evidence exposing the magnitude of the crisis: the Medicare incentive, the explosive growth of procedures in clinics and the potential for inappropriate treatment. Most critically, he warned about the risk of patient harm. In recent years, researchers have found that patients in early stages of vascular disease had less than a 2% risk of amputation after five years. However, with aggressive interventions, that risk could surge up to 5% or even 10%.
“The problem is that these behaviors — unindicated early interventions and overuse of unproven technologies — still have costs and more often than not, those costs are borne by our patients,” he said. “We can and should do better, otherwise we are also enablers.”
The issue has magnified into a crisis that has splintered the specialities that conduct these procedures, which include interventional radiologists, cardiologists as well as vascular surgeons. Some physicians do not view overuse as an urgent problem and feel the recent academic attention unfairly stigmatizes private practice doctors.
“The majority of operators are doing the right thing,” said Dr. Jeffrey Carr, an interventional cardiologist and the founding president of the Outpatient Endovascular and Interventional Society, which represents physicians working in outpatient settings. “We need to call out the bad actors, but to cast a narrative that puts us all in the same arena is wrong.”
Other doctors recognize a need for considerable reforms.
CMS could reverse the change that kicked off the entire problem, some experts said, by reducing its outpatient reimbursement rates. “If you shut off the money, the whole thing will stop tomorrow,” Mukherjee, the Virginia vascular surgeon, said.
But such cuts might hurt doctors practicing responsibly and could even nudge the least scrupulous ones into higher gear to make up the financial difference. “You could incentivize people to do more procedures, and some of them may be inappropriate,” said Dr. Peter Lawrence, the former chief of vascular and endovascular surgery at the University of California, Los Angeles, who developed an outpatient center connected to the university.
More critical than payment cuts, Lawrence said, is greater oversight of office-based facilities. Many states don’t require doctors in those settings to have special vascular training or hospital privileges in case of complications, he said. “You could be a psychiatrist and do these procedures,” he said.
Many physicians also support improved data collection, particularly for newer technologies like atherectomy, to ensure that they’re not only safe but result in improved outcomes.
“Many of the vascular procedures that are done are relatively safe or can be done with good short-term results, but the failures are long term — it’s what happens in two to five years,” Lawrence said. “Unless you have a reimbursement system, which not only pays you for the initial procedure, but whether or not it’s durable, you can have procedures done in our society that have great short-term results but have poor long-term results.”
CMS could require physicians to participate in patient registries, said Dr. William Schuyler Jones, an interventional cardiologist and associate professor of medicine at Duke University School of Medicine. “That type of required reporting would make our system better,” he said, “and would ultimately put the onus on all of us to do more appropriate care.”
For Dormu, patients were the ones to prompt accountability, airing their grievances to the Maryland Board of Physicians. Among them was a woman who sought his care for excessive leg itching and said he tried to pressure her into an invasive artery scan. When she sought a second opinion, the doctor concluded that her itching likely stemmed from a reaction to an insect bite.
The medical board examined the records of 11 of Dormu’s patients. Two peer reviewers, board certified in vascular surgery, independently concluded that Dormu had performed “medically unnecessary and invasive vascular procedures” and failed to meet appropriate standards of care for 10 of the 11 patients, “exposing them to potential risks such as bleeding, infection, blood vessel injuries which could acutely or chronically worsen the patient’s circulation, and limb loss.”
One patient who sought Dormu’s care to evaluate blockages in their legs could walk a mile before treatment, but after the procedures, they could not walk at all.

Credit:
Shuran Huang for ProPublica
“There exists a substantial likelihood of risk of serious harm to the public health, safety, and welfare in Dr. Dormu’s continued practice,” the board’s executive director, Christine Farrelly, concluded.
Last October, the board found him in violation of state medical law, citing his overuse of procedures and his failure to uphold standards of care. It fined him $10,000, suspended him and put him under a two-year probation, during which he must be supervised and enroll in an ethics course.
Maryland Department of Health spokesperson Chase Cook said the agency’s Office of Health Care Quality, which is responsible for oversight of the state’s surgical centers and licensed Dormu’s current facility, was not aware of his sanctions nor the allegations of harm. The office “will follow-up in accordance with federal and state regulations,” Cook said.
Despite lacking an active license to practice medicine in Maryland, Dormu is still listed on his clinic’s website as the lead vascular surgeon, “currently available for office visits and in-patient consultations.”
When ProPublica called Dormu’s office to inquire whether he was still practicing, the receptionist said he was no longer seeing patients and that “Dr. Seibles” was providing all the same services. According to the Virginia Board of Medicine’s directory, Dr. Ayana Jonelle Seibles spends 20% of her time practicing at Dormu’s center in Maryland.
An emergency medicine physician who does not have specialty training in vascular surgery, Seibles appears to have a close relationship with Dormu; according to county property tax records, they have owned a home together since at least 2017. Seibles did not respond to ProPublica’s questions that were sent by email.
In a lawsuit deposition last month, Dormu said that he stopped doing surgery this year as a “personal choice.” When asked the name of his supervisor, he stated that he couldn’t recall it. He also couldn’t recall how many times he had been sued for malpractice, any of the details of the cases, nor the names of the attorneys representing him. He also couldn’t specify how many atherectomies he had performed, only estimating that he had done more than 100.
According to Medicare data, over the past decade, he has done at least 3,400.
For most of his life, Rosenberg trusted doctors; his own father was one. But the mechanic has lost faith in medicine. Memories of his 2017 amputation have been largely buried by the trauma, but he recalls lying in his hospital bed after the operation, the remnants of his left leg wrapped in a cloud of white bandages. “Life isn’t supposed to turn out like this,” he said.
He was discharged to his three-story colonial home, where two steps led to the front door and 13 steps gave way to the second floor; he could only ascend them by crawling backward. Eventually, he sold the house and his family moved into a flat, ranch-style home.
He tried to maintain his auto shop, relying on his wife and teenage stepson to help out. But with his limited mobility, first in a wheelchair and later maneuvering with his prosthetic and a cane, he could not repair cars like he used to and was forced to sell his business and retire.
Before, he could get dressed and out the door in less than 30 minutes; it now takes more than an hour. He used to prepare meals for his family, but after, his stepson had to learn how to cook. In the months following the surgery, he often fell asleep by 7:30 p.m., tired from carrying his body around all day. Discomfort would awaken him by 4 a.m.
Half of his days are now spent navigating the complex web of amputee providers, arguing with insurance agents, attending physical therapy and meeting with specialists to keep his vascular system in check.
Above all, managing the pain has remained a lingering burden. Even though he lost most of his left leg, its memory has been indelibly burned into his brain, haunting him like a phantom. Sometimes the bottom of his missing foot itches or a jolt surges down his absent calf.
“And there’s nothing anyone can do about it,” he said, “because it’s not there.”
Do You Have Experience With Peripheral Artery Disease? Have You Had a Procedure on Your Leg? Tell Us About It.
Some doctors may be overusing a procedure to clear out clogged arteries in legs, potentially leading to amputations. We need your help connecting with patients, including those who may not know they have had an atherectomy.
[ad_2]
Source link