[ad_1]
Many hospitals and health systems realize they need to develop and implement an ASC plan. But knowing at the outset of the process how an ASC will fit into your broader organizational vision will make for better decision-making later on.
This means understanding why your hospital or health system needs an ASC plan to begin with, determining how many ASC ORs and procedure rooms you will need, and understanding the value ASCs will bring to your organization.
Hospital executives need to reflect on the following questions as they consider their ASC strategy:
- Are your hospital ORs and procedure rooms at capacity or underutilized?
- Has surgery migrated out of the hospital to competing ASCs?
- Will you be cannibalizing existing surgery and procedural volume that is in the hospital by developing an ASC?
- Are your physicians aligned? Are you having difficulty recruiting and retaining surgeons because you do not have an ASC site-of-service or partnership opportunity?
- Have physicians departed because you do not have an ASC?
- Are payers denying benefits to patients who need outpatient surgery that can be performed in an ASC?
- Are payers redirecting your cases to surgeons who have access to an ASC?
- Does an ASC strategy allow you to enter into secondary markets and create opportunity for accretive value?
- Does an ASC strategy in your primary market require decanting surgery and procedural volume that cannot be replaced due to the absence of backfill volume?
While there are many components that will contribute to the success of your ASC plan (see figure 1), pursuing the six steps detailed below should set your organization up for success.
FIGURE 1: Key Steps for ASC Development
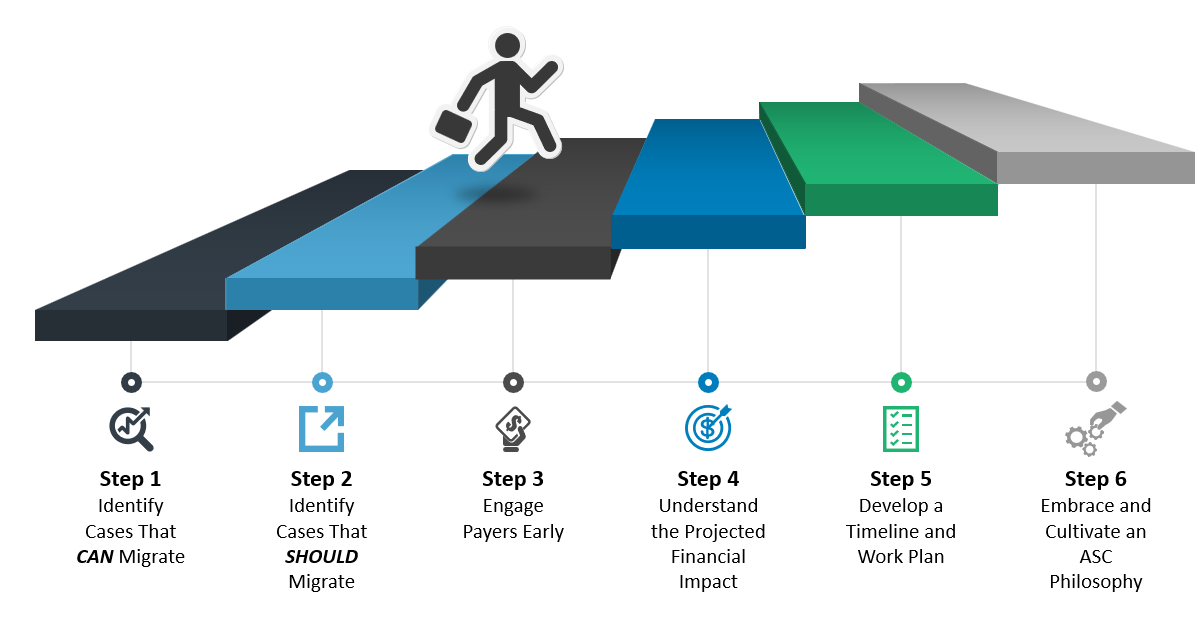
Step 1: Identify Cases that CAN Migrate
Start by conducting a site-of-service case volume analysis to evaluate the surgical and procedural case volume that is ASC eligible and performed in the hospital setting. Many factors should be considered, such as the CMS and commercial payer covered procedure lists (CPLs), ASC rules and regulations, patient selection criteria, comorbidities, and market conditions. By identifying the ASC-eligible cases, you can proceed with the process of optimizing the cases’ site of service and existing hospital assets.
This takes time and is complex, especially without ASC expertise in the planning process. Key considerations and factors beyond the payer-approved CPLs must be factored into the assessment, such as comorbidity factors, length of stay, and access to equipment (e.g., robotics) that may be required to perform the cases. Hospitals and health systems that do not have ASC expertise often work with an outside subject matter expert to facilitate this analysis.
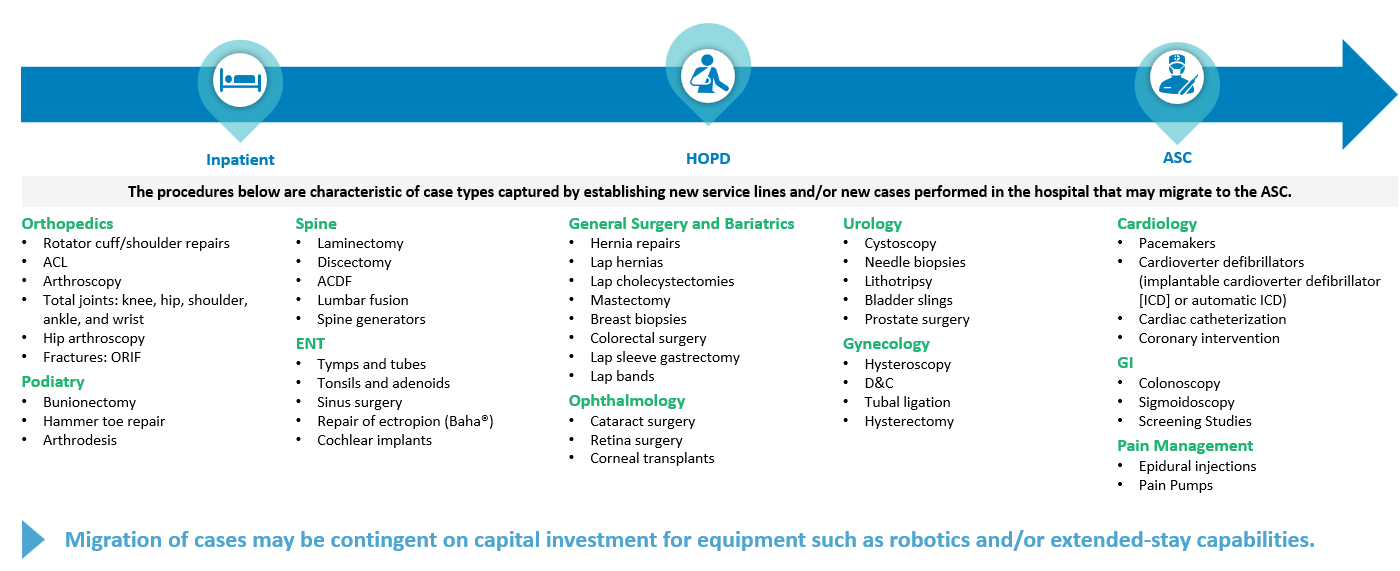
In addition to identifying cases commonly performed in an ASC setting, proactive organizations identify and plan for cases most likely to be performed in an ASC in the future (see figure 2).
FIGURE 2: Surgery Migration Trends
Step 2: Identify Cases That SHOULD Migrate
Just because cases are eligible to migrate doesn’t necessarily mean they should. This piece of the ASC planning process requires identifying key stakeholders and physician champions who will provide input from both a business and clinical standpoint. For instance, surgeons may not be comfortable performing some procedures in an ASC setting, or there may be limitations to accessing equipment that limit the opportunity for migration. Another key consideration is the broader financial impact of moving profitable cases out of a hospital OR and into an ASC.
Evaluating ASC-eligible cases starts with performing a thorough site-of-service assessment (with input from surgeons). This will an allow an organization to ultimately determine the feasibility and financial impact of cases that will and/or should migrate to an ASC.
Step 3: Engage Payers Early
More often than not, commercial payer contract rates will have a material impact on the financial feasibility of an ASC. So determining the opportunity for reasonable and appropriate reimbursement, and ensuring the ASC has optimal managed care rates, requires payer due diligence and initiating payer discussions early in the ASC development process.
Often, organizations invest time and money planning for their new ASC without being proactive with the payers. Assess opportunities to add ASCs to the hospital or health system commercial payer contracts, and build the business case for reducing the total cost of care. Being proactive with the payer is critical; hospitals and health systems that aren’t soon discover that the rates they receive from payers do not support developing their ASC.
It is also important to consider ASC partnership structure and how equity position and certain aspects of management control can impact the hospital’s position with the payer with respect to ASC rates. Being proactive and engaging with payers early on is a key component of the ASC strategy and planning, and can have material implications on the feasibility of the ASC.
Successful organizations prepare for success with ASC managed care contracting and strategy 9 to 12 months before the ASC is expected to open (or sooner). It is critical the hospital or health system evaluate the implications of migration, develop a business case, and establish a business structure that allows for success with payers.
Step 4: Understand the Financial Impact
Developing an ASC and understanding the projected financial impact is more than just identifying the up-front capital requirements and projecting EBITDA. A mistake many hospitals and health systems make is to invest time understanding the financial performance of the ASC without also evaluating the financial impact.
Moving cases out of a hospital into an ASC will inevitably impact a hospital’s financial performance if there is no opportunity to backfill cases. If the hospital or health system has opportunity to backfill, it will be important to consider the impact on the payer mix and the types of cases that will be performed that replace the procedures that are anticipated to migrate. This is a critical component of the managed care planning and strategy as well, and should also be considered with respect to the equity position the hospital and or health system has in an ASC joint venture.
Step 5: Develop a Timeline and Work Plan
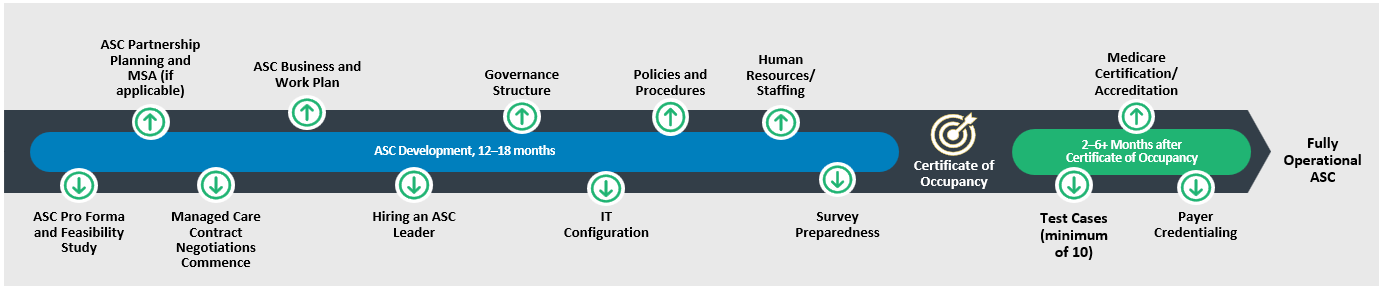
A solid ASC plan builds in enough lead time to perform the analyses necessary to deliberate and make critical decisions, as well as the flexibility to account for unexpected delays. Typically, organizations should plan on the development process taking 12 to 18 months; this is highly dependent on whether the ASC is a buildout of an existing space or if the ASC requires the development of a new building from the ground up.
There are many components and milestones that can impact the timeline and ultimately the pro forma and operating work plan. It is important to account for delays, such as:
- The timeline between certificate of occupancy, a state survey, and an accreditation/Medicare survey.
- Payer credentialing and contracting.
- Recruitment of an ASC leader and staffing.
Figure 3 provides an example of an ASC development timeline of a de novo ASC, and some important milestones.
FIGURE 3: ASC Development Timeline
Step 6: Embrace and Cultivate an ASC Philosophy
One reason ASCs typically operate more efficiently than hospitals is the ASC’s operational philosophy, culture, and “can do” attitude. When developing your health system’s ASC plan and strategy, it is important that this philosophy is present at all phases of development to ensure operational efficiency and excellence and care delivery that meets and exceeds ASC standards while achieving high levels of patient, physician, and employee satisfaction. Involving ASC experts in both the planning and execution stage of your ASC strategy will increase the likelihood of your strategy’s success.
Stay tuned for our next blog on the key success factors for implementing your ASC plan.
This article was written by Naya Kehayes, Emily Lopez and Dan Cosentino.
[ad_2]
Source link